SPL
Stabiliz Polymer Locking (SPL®) Technology
The first truly dynamic plate and screw technology: a system that changes with body during the course of fracture healing.
Concept
THE PROBLEM
Studies examining locked plating indicate reasons for concern due to the reported rates of non-unions and delayed unions. Recently, these healing difficulties have been reported in up to 23% of distal femur, 15% of distal tibia and 6% of proximal humerus fractures. [1, 2, 3]
Previous studies have shown that the high overall rigidity of locked plating can contribute to healing difficulties by inhibiting interfragmentary motion. [4] Under compression, rigid locking plates asymmetrically bend, limiting cortical motion. This rigidity may produce stress shielding across the fracture site, contributing to nonunions, which may result in implant fatigue and failure under repetitive loading. [4, 5]
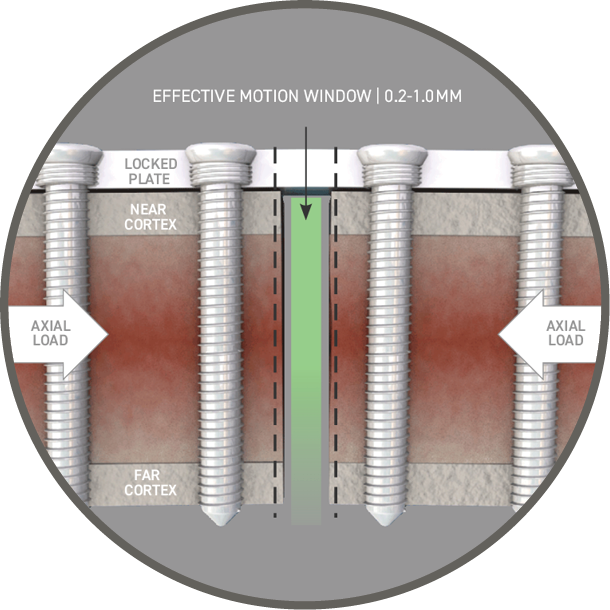
Illustration depicting how the rigidity of locked plating inhibits sufficient interfragmentary motion.
THE SOLUTION
SPL® screws function in a manner similar to conventional locking screws at implantation and reduce construct stiffness over time, promoting interfragmentary motion. Delayed dynamization has shown enhanced healing when compared to constantly flexible fixation or early dynamization in animal models. [6, 7]
Clinically, favorable outcomes have been reported with dynamization of intramedullary nails between 3-5 months. [8, 9] In the presence of delayed unions, dynamization initiated between months 3 to 6 has been associated with higher bone union success rates. [10]

Illustration depicting how the polymer SPL® locking mechanism transforms with time.
Technology
SPL® locking screws are stainless steel with a PLGA locking mechanism. The system is implanted using conventional plating techniques, including bi-cortical screw fixation. The polymer locking mechanism resorbs over four to six months, while the screw head remains in contact with the plate. Under load, the screw moves relative to the plate to create interfragmentary motion at the fracture site.

Illustration depicting how, with time, SPL Locking Screws promote interfragmentary motion at both near and far bone cortices.
REDUCED STIFFNESS
Axial stiffness decreased up to 57% after resorption of the SPL® locking mechanism. Decreases in fixation stiffness from 29-86% have improved rates of fracture healing and remodeling in animal models. [4, 6, 13]

SPL® locking screw constructs show stiffness comparable to traditional locking screws at implantation. With time, SPL® screw constructs show a statistically significant reduction in stiffness, promoting interfragmentary motion.
INCREASED MOTION
SPL® screws created significant increases in micromotion at the near and far cortices after resorption. Interfragmentary motion between 0.2 to 1 mm has been shown to promote secondary bone healing and remodeling. [13, 14]
References
HENDERSON C, ET AL. Healing Complications Are Common After Locked Plating for Distal Femur Fractures. Clin Orthop Relat Res. (2011) 469:1757–1765
KHALSA A, ET AL. Distal tibia fractures: locked or non-locked plating? A systematic review of outcomes. Acta Orthopaedica. 2014; 85 (3): 299–304
CLAVERT P, ET AL. Pitfalls and complications with locking plate for proximal humerus fracture. J Shoulder Elbow Surg. 2010 Jun;19(4):489-494
BOTTLANG M, ET AL. Effects of construct stiffness on healing of fractures stabilized with locking plates. J Bone Joint Surg Am. 2010;92 Suppl 2:12-22
STRAUSS EJ, ET AL. The current status of locked plating: The good, the bad, and the ugly. J Ortho Trauma. 2008;22:479-486
CLAES, ET AL. Late dynamization by reduced fixation stiffness enhances fracture healing in a rat femoral osteotomy model J Orthop Trauma. 2011;25:169-174
WILLIE, ET AL. Temporal variation in fixation stiffness affects healing by differential cartilage formation in a rat osteotomy model. Clin Orthop Relat Res. 2011;469:3094-3101
GROSSE A, ET AL. Treatment of fragments, loss of bony substance and pseudarthrosis of femur and tibia using screw fixation (40 cases). Rev Chir Orthop Reparatrice Appar Mot. 1978;64S:33-35
RIQUELME, ET AL. Treatment of the femoral and tibial fractures with Grosse and Kempf locking nails. Clin Orthop Relat Res. 1992:86-89
HUANG KC, ET AL. Evaluation of methods and timing in nail dynamisation for treating delayed healing femoral shaft fractures. Injury. 2012;43:1747-1752
ROBERTS, ET AL. Biomechanical evaluation of locking plate radial shaft fixation: Unicortical locking fixation versus mixed bicortical and unicortical fixation in a sawbone model. J Hand Surg Am. 2007;32:971-975
FULKERSON, ET AL. Fixation of diaphyseal fractures with a segmental defect: A biomechanical comparison of locked and conventional plating techniques. J Trauma. 2006;60:830-835
GOODSHIP, ET AL. The influence of induced micromovement upon the healing of experimental tibial fractures. J Bone Joint Surg Br. 1985;67:650-655